International Journal of Cardiovascular Sciences. 28/jul/2021;35(2):293-6.
Commotio Cordis Secondary to Aggression
Luisa Gonçalves
![]() , Inês Pires
, Inês Pires
![]() , João Santos
, João Santos
![]() , Joana Laranjeira Correia
, Joana Laranjeira Correia
![]() , Davide Moreira
, Davide Moreira
![]() , Inês Almeida
, Inês Almeida
![]()
Case report
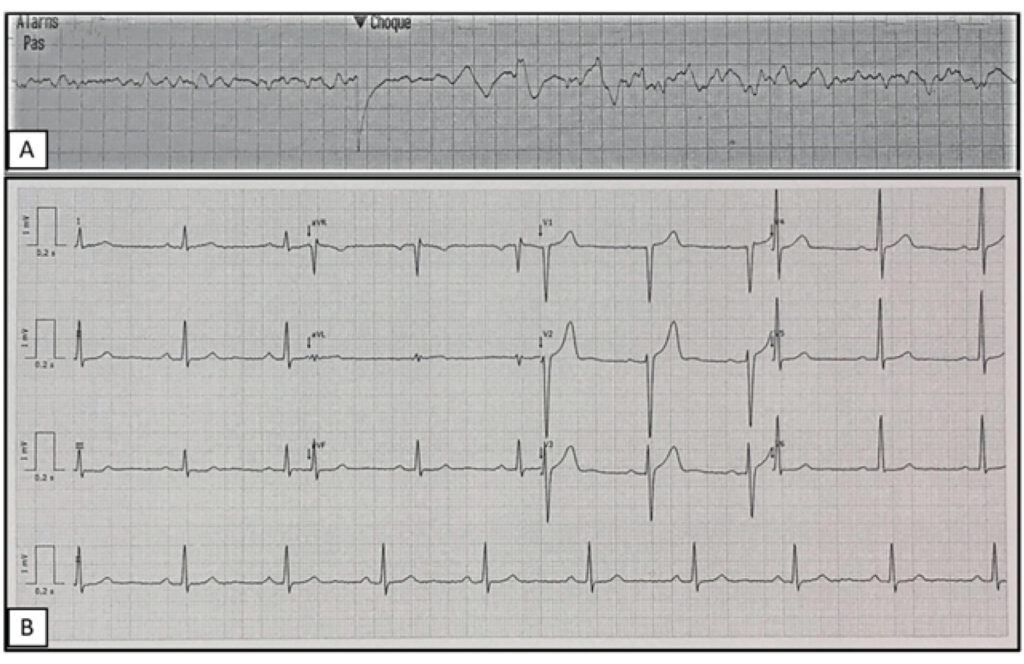
A 35-year-old man was admitted following a recovered cardiorespiratory arrest. He was attacked by another man with multiples blunts by a wood stick in the chest and head. An eyewitness statement indicated that the victim had lost consciousness and collapsed after being hit in the chest. He was in cardiac arrest, and a nearby healthcare professional provided first aid with cardiopulmonary resuscitation. The first electrocardiogram (ECG) rhythm strip, fifteen minutes later, identified ventricular fibrillation (VF) (). Sixteen electrical shocks were delivered, always with VF, before restoration of sinus rhythm and circulation. A 12-lead-ECG revealed sinus rhythm without ST deviations and a corrected QT interval of 414 msec. On admission, he was under ventilatory support, with a heart rate of 80 beats per minute, blood pressure of 121/70mmHg, and no signs of shock. There was no previously known medical condition, besides being an active smoker and a binge drinker, and no family history of early coronary disease, cardiomyopathy, or sudden death. He was under the influence of alcohol, as was confirmed by blood tests (blood alcohol level of 1.31g/L), and had a discretely elevated cardiac troponin-T of 0.9ng/ml (normal range, 0 to 0.08 ng/ml). The remaining analyzes, cranial and cervical CT scan, chest X-ray, and abdominal eco FAST were normal. An initial echocardiogram in the emergency department demonstrated normal-sized chambers and global ventricular systolic dysfunction explained by a prolonged cardiac arrest. He was admitted to the intensive care unit for post-resuscitation care with therapeutic hypothermia and temporary ventilatory support. At 48 hours of admission, there was a normalization of systolic function with a normal ejection fraction by echocardiogram (). Coronary angiography excluded coronary disease (). Serial electrocardiograms were not suggestive of an arrhythmogenic substrate (). The sudden cardiac arrest was assumed secondary to a commotio cordis (CC), and for this reason, the patient was not proposed for an implantable cardioverter-defibrillator (ICD). The clinical outcome was favorable, and the patient was discharged. He remained asymptomatic during three years of follow-up, with normal ECG, echocardiogram with strain-rate imaging, exercise stress test, and 24-hour-Holter. During mid-term follow-up, a cardiac magnetic resonance imaging (MRI) showed normal-sized chambers, global and regional function, and no myocardial edema or myocardial scar by late focal hyperenhancement (-).
[…]
1.145